
Bioelectronic Devices for Immune Protection and Oxygenation of Islets In Vivo- Siddharth Krishnan PhD -Stanford
Pregame: Ahead of the May 19 talk

TheSugarScience T1D Th1nk Tank
📅 Registration
Date: Tuesday, May 19, 2026 · 11:00 AM Pacific · 2:00 PM Eastern Format: Free virtual seminar for the global T1D research community — scientists and clinicians are welcome.
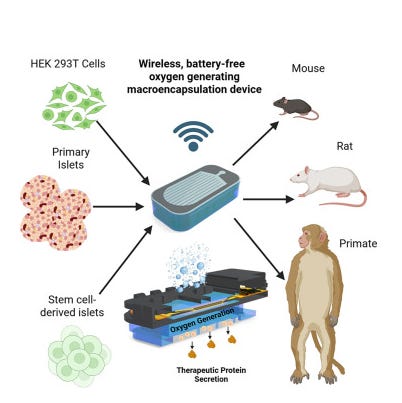
Figure adapted from DOI: 10.1016/j.device.2026.101084
👤 About the Speaker
Siddharth Krishnan, PhD is an Assistant Professor of Electrical Engineering — and by courtesy, of Bioengineering and Materials Science and Engineering — at Stanford University. He received his BS and MS from Washington University in St. Louis and his PhD from the University of Illinois at Urbana-Champaign, before joining the Koch Institute for Integrative Cancer Research at MIT as a K99-funded Research Scientist, also affiliated with Boston Children’s Hospital.
His work sits at the intersection of electronics, materials science, and cell engineering — developing bioelectronic devices that solve fundamental biological problems in cell therapy. For T1D specifically, his lab focuses on three linked challenges: building wireless, battery-free oxygen-generating implants for immunosuppression-free islet transplantation; engineering GLP-1 secreting cell implants as long-term alternatives to injectable therapy; and developing wireless-triggered glucagon delivery devices for hypoglycemia rescue. He has been recognized with a Terman Faculty Fellowship at Stanford, a JDRF Postdoctoral Fellowship, the 2019 Illinois Innovation Prize, a graduate medal from the Materials Research Society, and placement on MIT Technology Review’s Global Innovators Under 35 list. His co-first author on today’s paper is Matthew Bochenek, PhD — a prior TSS guest and a central figure in this research program.
01 · The Paper
“Wireless Battery-Free Oxygenation Devices Enable Extended Immunosuppression-Free Islet Transplantation in Minimally Invasive Sites” Krishnan SR, Bochenek MA, Pan J, Liu C, … Langer R & Anderson DG · Device, 2026 DOI: 10.1016/j.device.2026.101084
Every encapsulated islet transplant faces the same engineering paradox: the membrane that protects cells from immune rejection also cuts them off from the blood supply that delivers oxygen. Pancreatic islets are among the most metabolically demanding tissues in the body — they consume oxygen at rates that exceed most other cell types — and without a blood supply, islets packed inside a subcutaneous device die within days from hypoxia. The field has struggled with this for decades. Krishnan and Bochenek’s paper is the most credible engineering solution yet: a wireless, battery-free, implantable device that generates its own oxygen electrochemically, in situ, powered wirelessly through the skin — and that keeps islets alive and functional at the subcutaneous site for significantly extended periods without any immunosuppression.
The device — called the HOBIT (Hybrid Oxygenation Bioelectronics for Implanted Therapy) system in companion work, and refined here into its most durable iteration — operates through electrochemical water splitting. An electrode splits water molecules into hydrogen and oxygen; the oxygen diffuses directly to the encapsulated islet chambers below, while hydrogen is safely vented. The critical engineering advance in this paper over the team’s 2023 PNAS proof-of-concept is durability: the devices were made substantially more waterproof and crack-resistant through improved encapsulation materials, and the wireless power electronics were optimized to deliver significantly more power to the oxygen generator — extending functional device lifetime from approximately one month to substantially longer in vivo.
The device is powered by an external antenna worn on the skin that transfers energy via resonant inductive coupling — the same principle used in wireless phone charging — to a flexible circuit embedded in the implant. There are no batteries, no refillable reservoirs, no percutaneous ports, and no toxic byproducts. The entire system is designed for minimally invasive subcutaneous delivery — a critical feature for SC-islet programs that require retrievability and monitoring.
The headline results: in immune-competent diabetic animals, HOBIT-supported islet implants maintained normoglycemia for extended durations without immunosuppression — substantially exceeding what is achievable with encapsulation alone. Islet viability and glucose-stimulated insulin secretion were preserved at high cell densities (~1,000 islets/cm²) that would be lethal under passive oxygen diffusion conditions. The paper includes systematic in vitro characterization of device performance across a range of ambient oxygen concentrations, and in vivo validation in freely moving, awake animals — the most clinically relevant testing condition.
Tags: bioelectronics · oxygen generation · encapsulation · subcutaneous transplantation · wireless power · immunosuppression-free · islet transplantation · SC-islets · water splitting · HOBIT · cell therapy · T1D · implantable device
02 · Why This Matters
For scientists: The oxygen delivery problem in encapsulated cell therapy has been recognized for more than 30 years, but prior solutions — oxygen-permeable membranes, perfluorocarbon oxygen carriers, externally pressurized oxygen chambers — all require either frequent refilling, percutaneous access, or accept fundamentally limited oxygen delivery. Krishnan’s electrochemical approach generates oxygen continuously and indefinitely from the water already present in surrounding tissue, powered wirelessly through the skin. This removes the oxygen constraint without any of the logistical or safety limitations of prior approaches. Combined with the improved waterproofing and crack resistance that extends device lifetime, this is the first encapsulated islet platform with a credible path to months- to years-long function in the subcutaneous space.
For clinicians: The subcutaneous site is the only currently viable location for retrievable SC-islet transplantation — a non-negotiable requirement for regulatory approval of SC-islet therapies given their novel nature. Vertex’s Zimislecel uses the intraportal route with immunosuppression; programs pursuing immunosuppression-free, retrievable SC-islet transplantation have no choice but the subcutaneous space, where oxygen tension is inherently lower and fibrosis compounds the problem. HOBIT directly solves both. For patients, the clinical vision is compelling: a quarter-sized implant placed subcutaneously in a minimally invasive procedure, powered daily by a wearable patch on the skin, maintaining insulin independence without immunosuppressive drugs. The manufacturing and regulatory path for a combined cell-device product is complex — but the biological proof of concept is now firmly established.
The broader picture: This paper is part of a broader convergence between bioelectronics and cell therapy that is one of the most exciting frontiers in medicine. The same wireless power and electrochemical engineering principles Krishnan applies to oxygen generation could in principle be used to deliver electrical stimulation to enhance beta cell maturation (as in Alvarez’s nanoelectronics work), to trigger drug release, or to close the loop with continuous glucose sensing. The HOBIT device is not just an oxygen solution — it is a platform architecture for programmable, wireless, in vivo control of implanted cell therapies.
03 · Four Questions We Will Ask the Speaker
Q1. The key advance over your 2023 PNAS device is extended durability through improved waterproofing and crack resistance. What was the primary failure mode of the earlier device — was it water ingress to the electronics, mechanical fatigue of the oxygen-generating electrode, or delamination of the encapsulant — and how confident are you that the current iteration has eliminated that failure mode for a multi-year clinical timeline?
Q2. The external antenna must be worn on the skin directly over the implant to transfer power. In a real patient, compliance with daily antenna wear will vary — what happens to the islets during gaps in power delivery? Is there a safe minimum daily charging duration, and do the islets tolerate intermittent hypoxia if the patient forgets to wear the antenna for a day or two?
Q3. Electrochemical water splitting generates hydrogen as well as oxygen. You state hydrogen is safely vented — but in a subcutaneous implant surrounded by tissue, where exactly does the hydrogen go, and is there any evidence of hydrogen bubble accumulation, local pH changes, or tissue irritation at the implant site over extended periods?
Q4. The HOBIT device currently encapsulates cadaveric or xenogeneic islets in proof-of-concept studies. For SC-islet products specifically — which need to meet regulatory release criteria for cell viability, identity, and potency — does the device loading process and the electrochemical environment inside the implant chamber alter SC-islet function or transcriptional identity, and how will you validate that the cells inside the device at 6 or 12 months are still performing as intended?
04 · Four Key Associated Papers
1. Krishnan SR, Liu C, Bochenek MA, … Langer R & Anderson DG (2023) A wireless, battery-free device enables oxygen generation and immune protection of therapeutic xenotransplants in vivo PNAS, 120(40):e2311707120 · PMC → The foundational proof-of-concept paper for the wireless oxygen-generating encapsulation device — the direct scientific predecessor to today’s paper, demonstrating one-month normoglycemia in immune-competent animals with xenogeneic islets and no immunosuppression.
2. Krishnan SR, Liu C, Bochenek MA et al. (2026) Design of a wireless, fully implantable platform for in-situ oxygenation of encapsulated cell therapies Device · Read paper → The companion HOBIT architecture paper published simultaneously — provides the detailed engineering design framework, in vitro performance characterization, and systems-level description of the wireless power and electrochemical oxygenation platform.
3. Colton CK (2014) Oxygen supply to encapsulated therapeutic cells Advanced Drug Delivery Reviews, 67–68:93–110 · PubMed → The canonical bioengineering framework for oxygen transport in encapsulated cell therapy — establishes the theoretical basis for why passive diffusion fails at clinically relevant cell densities and why active oxygen supplementation is necessary, motivating the HOBIT approach.
4. Shapiro AMJ, Thompson D, Donner TW et al. (2021) Insulin expression and C-peptide in type 1 diabetes subjects implanted with stem cell-derived pancreatic endoderm cells in an encapsulation device Cell Reports Medicine, 2(12):100466 · PubMed → The first-in-human encapsulated SC-islet transplant study — establishes the clinical benchmark for what a device-based SC-islet therapy must achieve and the limitations of encapsulation without active oxygen supplementation that the HOBIT device is designed to overcome.
05 · Four Videos to Watch First
▶ T1D Th1nk Tank: Matt Bochenek, PhD — MIT Bochenek is the co-first author on today’s paper and a prior TSS speaker — watch this first for essential background on the MIT encapsulation and oxygen delivery program that Krishnan’s device directly builds upon.
▶ Ask the Expert: Alex Abramson, PhD — Georgia Tech Abramson works on ingestible and implantable drug delivery bioelectronics — the closest parallel engineering discipline to Krishnan’s wireless implantable device platform, and essential context on the state of the art in bioelectronic cell therapy delivery.
▶ Ask the Expert: Josh Doloff, PhD — Johns Hopkins School of Medicine Doloff works on biomaterial strategies for improving islet engraftment at extrahepatic sites, including fibrosis mitigation — directly relevant to the subcutaneous implant environment where the HOBIT device operates.
▶ Ask the Expert: Jessica Weaver, PhD — ASU Weaver develops biomaterial and encapsulation strategies to protect transplanted islets from immune attack — the immune protection side of the same dual challenge (immune isolation + oxygenation) that Krishnan’s device addresses simultaneously.
TheSugarScience · Expediting a cure for T1D by curating the scientific conversation · thesugarscience.org
This is a great reminder that living therapies need infrastructure. The cells may be the treatment, but the device has to keep them alive, protected, and functional. Do you think the future of cell therapy will depend as much on bioengineering as on stem cell biology?